
The International Basic Safety Standards (GSR Part 3) requires specialized radiation protection measures for female workers in medical facilities that utilize ionising radiation (diagnostic radiology, nuclear medicine, image guided interventional procedures and radiotherapy facilities) to protect both the worker’s health as well as the health of any unborn children in the case of pregnancy.
The IAEA launched an anonymous survey among its Member States to understand radiation protection situations of female workers around the world.
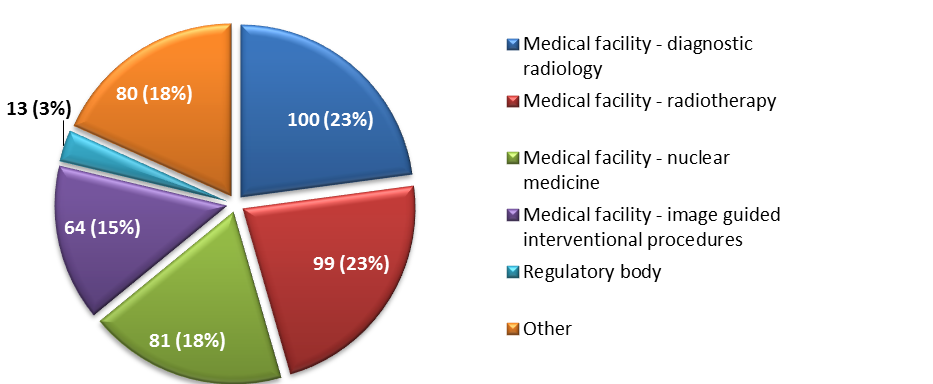
By the end of November 2016, 182 participants from 61 countries from all regions in the world responded to the survey. Here is their distribution by type of represented institution and profession:
All graphs show the number of responses per category and their percentage (in brackets).
Conclusions
The survey demonstrated big variations in policies, procedures and practices among different Member States and different facilities, prompting for more guidelines and actions.
There is no requirement in the International BSS, GSR Part 3 for a female worker to notify the licensee that she is pregnant, but it is necessary that female workers understand the importance of making such notifications so that their working conditions may be modified accordingly. GSR Part 3 establishes requirements for the employers, in cooperation with registrants and licensees, to provide female workers with appropriate information in this regard (GSR Part 3, para. 3.113 (b)).
The employer of a female worker, who has been notified of her suspected pregnancy, is required to adapt the working conditions in respect of occupational exposure so as to ensure that the embryo or fetus is afforded the same broad level of protection as is required for members of the public (GSR Part 3, para. 3.114).
The limitation of the dose to the embryo or fetus does not mean that pregnant women should avoid work with radiation, but it does imply that the employer should carefully review the exposure conditions with regard to both normal exposure and potential exposure. A possible solution includes reassignment of a pregnant worker to a location that may have lower ambient dose equivalent; for example, from fluoroscopy to radiography or to CT. Such reassignments should be accompanied by adequate training. In nuclear medicine, a pregnant worker may be restricted from spending a lot of time in the radiopharmacy or working with solutions of radioiodine. The main risk with radioiodine is that it crosses the placental barrier and concentrates in the fetal thyroid. A further consideration is the need to avoid having pregnant workers respond to an accident such as a radioactive spill, or in radiotherapy with a cobalt-60 unit or an HDR brachytherapy unit.
When the dose limit of 1mSv is applied for the embryo or fetus, the reading of the dosimeter may overestimate the dose to the embryo or fetus by a factor depending on the energy and type of the incident radiation (by a factor 10 for low energy X rays and by a factor of about 2 for cobalt-60 and MeV X rays). The dose to the fetus should be monitored using an additional dosimeter that is appropriately positioned. Information, advice and, if indicated, counselling for pregnant workers should be made available.
The survey will be closed on 15 January 2017. Thank you for answering the questions.
Please feel free to forward this survey to your colleagues.
